Click here for a downloadable PDF copy of this commentary
Going Beyond the Surgeon General’s Report: Redefining the Goals of Prevention, Treatment and Recovery
The close of 2016 saw the release of Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health, providing sorely needed direction to a nation grappling with a serious drug epidemic. [1] We at the Institute for Behavior and Health, Inc. (IBH) are particularly interested in how close this landmark Report comes to our recommendations about the fundamental goals of youth substance abuse prevention and treatment for substance use disorders. For young people under the age of 21, IBH defines the goal of substance abuse prevention as no use of any alcohol, tobacco, marijuana or other drugs for reasons of health. Similarly, IBH defines the goal of substance abuse treatment as sustained recovery with a standard outcome measure of treatment of no use of such substances for at least five years.
We recall that the impact of the 1964 Surgeon General’s Report, Smoking and Health, was profound. It resulted in a slow cascade over several decades of legal sanctions on the advertising, sale and place of consumer use of tobacco products and an impressive multifaceted and multitargeted public education campaign that conveyed scientific knowledge about the severe negative health consequences of tobacco (nicotine) use. The result was a sustained decline in the use of all tobacco products coupled with a temporarily robust smoking cessation and treatment movement. Today we take for granted that Americans of all ages, even the very young, know that tobacco use is unhealthy and that its use is actively discouraged. Why do we not do the same with other substances of abuse such as alcohol and marijuana, the two most widely used drugs that are typically precursors to other drug use including nonmedical use of prescription opioids and heroin? This Commentary discusses these important issues.
The Surgeon General’s Report on Prevention
We commend the Office of the US Surgeon General for its clear message that substance use disorders are preventable.
The substance abuse prevention programs described in the Report for ages 0-10 concentrate on reducing risk factors by strengthening parent-child relationships, improving parenting skills and encouraging children’s problem solving skills. The expectation is that such programs reduce substance use later in life. No information is provided about the health implications of substance use and no recommendation is made that youth refrain from any substance use for their health.
For substance abuse prevention for ages 10-18 the Report focuses on providing adolescents with “life skills” and “substance refusal skills”. It cites The Botvin LifeSkills Program which covers topics such as managing and reducing stress and anger and building healthy relationships as well as learning about the consequences of drug use and risk taking. However, the Report states that this program has little effect on marijuana and other drug use, though it may reduce drinking and polydrug use. The Report also mentions results of similar programs in rural settings that show little effect on substance use.
Many of the adolescent substance abuse prevention programs described in the Report focus on high-risk populations including youth with impulse control issues, aggressive behavior, and those from lower socio-economic backgrounds.
In considering substance abuse prevention programs for young adults over the age of 18, the Report focuses on preventing the progression of substance use to substance misuse or “problematic use”. These prevention programs include the use of screening, brief intervention and referral to treatment (SBIRT) in school and primary care settings.
The IBH Prevention Message
IBH defines the fundamental goal of substance abuse prevention as no use of any alcohol, tobacco, marijuana or other drugs for reasons of health. Today’s prevention efforts must go further than simply reducing risk factors and increasing protective factors, though these are both important. The key facts that most substance use disorders can be traced to early initiation of substance use [2] and that the vulnerable brain is still developing until about age 25 [3] place additional emphasis on the need for more specific and effective prevention. Prevention should provide brief, clear, age-appropriate messaging that any youth substance use is unhealthy as well as illegal. In fact it is specifically illegal for the young, because it is unhealthy. Consistent messaging should come from many sources including schools, communities, religious groups, physicians and other health care providers as well as the media. All have a stake in and responsibility for the healthy development of our nation’s youth. At present the prevention messaging to youth and their parents from these various sources is unclear, inconsistent or in some cases non-existent. The acknowledgement is almost non-existent that any substance use by youth is unhealthy.
While the Surgeon General’s Report considers high-risk youth as a specific target population, we contend that today’s substance use and resulting problems including addiction are “equal opportunity”. The modern drug epidemic is not isolated within populations traditionally viewed as high-risk nor is it concentrated in inner city disadvantaged communities. Communities across the country are struggling to reduce the terrible toll of substance abuse. The US Centers for Disease Control and Prevention (CDC) reports national increases in heroin use and related deaths for all demographic groups, particularly among non-Hispanic whites. [4][5] Armed with the knowledge that youth use of the purportedly “safer” drugs of alcohol, tobacco (nicotine) and marijuana are highly correlated with one another as well as the use of other illicit drugs [6], we emphasize that for youth the decision to use any one substance opens the door to the use of other substances. For that reason we contend that young people should make one decision not to use at all for reasons of health.
With broad cultural exposure to substances of abuse – from legal alcohol to the shifting legal status of marijuana to legal prescription medications – as well as possible exposure in the home by parents, siblings, friends and the media, educating parents early about preventing all substance use by their children is crucial. Both parents and their children’s health care professionals need to understand that the use of any substance is unhealthy and all of these adults are in important positions to advise youth explicitly to not to use any alcohol, tobacco, marijuana or other drugs for their health. Substance use prevention is healthy brain protection.
In a clinical report [7] and related policy statement [8] on screening, brief intervention and referral to treatment (SBIRT), the American Academy of Pediatrics emphasizes that no use is the ultimate health goal for young patients and encourages pediatricians to support the choices made by their patients to refrain from any use and when youth already are using substances to encourage them to stop using. At present, such action by physicians is uncommon.
School-based substance abuse prevention programs also have important roles to play in empowering youth to make the healthy choice to refrain from substance use. Already in some areas of the country prevention curricula are directed at 4th and 5th graders based on the premise that teaching young people about healthy decisions in the early school years is protective.
Consistent, age-appropriate substance abuse prevention messaging focused on the fundamental goal for youth of no use of alcohol, tobacco, marijuana or other drugs must be both available and easily located on websites frequently accessed by the public seeking scientific information about the health consequences of substance use. At present finding this health-focused goal on such website resources is difficult or impossible. Media campaigns using population cohort targeted platforms also should support this no-use for health prevention messaging.
From an early age and throughout adolescence young people should be educated about the importance of avoiding substance use so they are well-prepared before they have to make the choice whether or not to use.
There is a tendency on the part of some of even the most knowledgeable people to shrug off substance abuse prevention efforts as useless because “all kids experiment”. Anecdotal stories abound about educators and medical practitioners who sanction such “trivial” substance use behavior. It is important that parents and other adults, including prevention professionals, not assume either that most young people will try alcohol and other drugs or that a little use does not pose health risks.
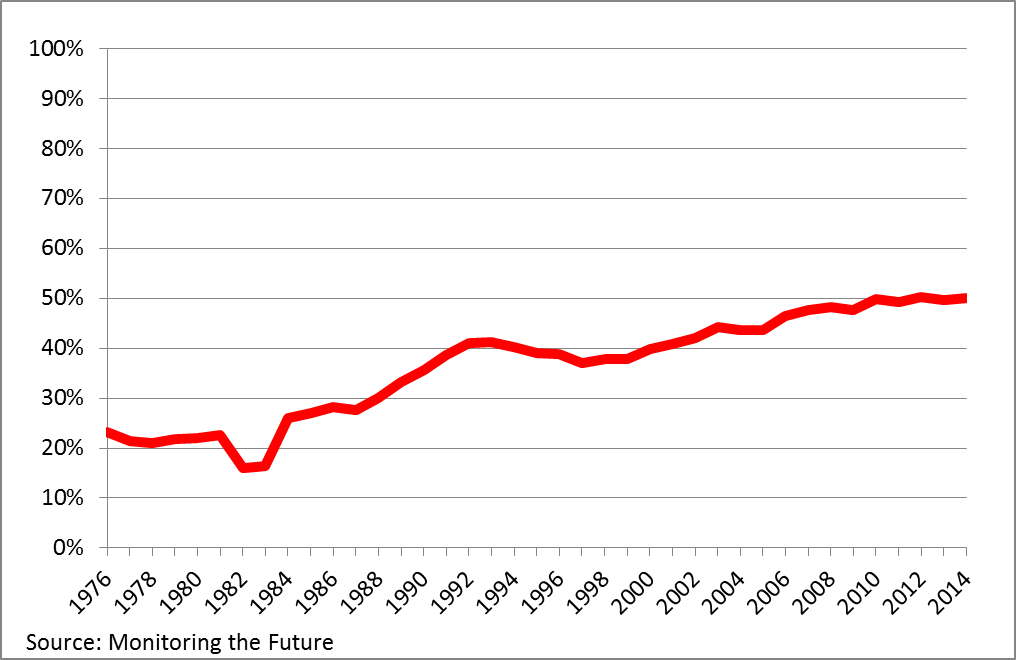
Using data from the nationally representative Monitoring the Future survey, IBH has shown that over the past three decades an increasing number of American high school seniors have abstained from using any alcohol, cigarettes, marijuana and other illicit drugs.[9] Among American high school seniors in 2015, 26% never, not even once in their lives, used any alcohol, tobacco, marijuana or other drugs and fully 50% have not used any alcohol, tobacco, marijuana or other drugs in the past 30 days. These new data on the growing population of youth who do not use drugs need to be publicized widely. New prevention strategies need to be developed that empower young people who do not use any drugs to talk with their peers about their healthy choices. Adults need to acknowledge and support this growing cohort of young people who are abstaining. Just as healthy eating and regular exercise are encouraged in the interest of health, so too can be an alcohol- and drug-free lifestyle.
Substance use disorders are entirely preventable when young people make the single decision not to use any substances of abuse. We hope that many more young people will continue to make this choice armed with information through new prevention efforts about how substance use negatively impacts health, and in particular, how it harms the developing brain.
The Surgeon General’s Report on Treatment and Recovery
Laudably, the Report stresses the importance of making long-term recovery the goal of substance abuse treatment. This ideal is expressed in a “continuum of care”, defined as “an integrated system of care that guides and tracks a person over time through a comprehensive array of health services appropriate to the individual’s need.” The full continuum of care promises to integrate specialty substance abuse treatment into the larger health care system, rather than treating it as an orphan outsider. Ideally health care would extend from primary prevention of the use of any substance through diagnosis of a substance use disorder, intervention and treatment to post-treatment long-term monitoring and intervention in case of relapse. Such a continuum holds the promise of drastically reducing not only the initiation of the use of alcohol and other drugs, but also addiction and subsequent relapse.
The Surgeon General’s Report does not provide a single definition of recovery but instead suggests several. For example, one definition is from the Betty Ford Institute’s Consensus Panel: “a voluntarily maintained lifestyle characterized by sobriety, personal health, and citizenship”. This definition highlights sobriety – no use of alcohol, marijuana and other drugs – as an essential element of recovery. Recovery, however, is more than abstinence from the use of alcohol and other addicting drugs. Recovery also includes meaningful character development and citizenship.
A less specific definition of recovery is that of the Substance Abuse and Mental Health Services Administration (SAMHSA): “a process of change through which individuals improve their health and wellness, live self-directed lives, and strive to reach their full potential”. Of the two definitions presented in the Report, IBH favors that of the Betty Ford Center which matches the standard of 12-step fellowships including Alcoholics Anonymous and Narcotics Anonymous.
The IBH Standard of Treatment and Recovery
IBH defines the fundamental goal of substance abuse treatment as sustained recovery, with a standard outcome measure of treatment of no use of such substances for at least five years. It is unfortunate that the Surgeon General’s Report is not explicit about the long-term sustained sobriety that characterizes recovery, considering the high prevalence of relapse after entering treatment among individuals with substance use disorders. Such relapse is similar to rates for many other chronic illnesses like diabetes and hypertension. [10] Of particular concern is the risk of overdose and death that awaits individuals with opioid use disorders who cut back their use of heroin or other opioids. Cutting back results in a loss of tolerance to a certain level of previous use, and overdose results when use is resumed at the previous dose level.
For individuals with substance use disorders, any use, even low levels of alcohol and drug use, puts them in danger of a severe relapse. There are numerous elements that support recovery: substance abuse treatment, 12-Step fellowships or similar peer-based recovery support, or an individual decision to stop using. For many individuals in recovery, a “sobriety date”, the last date on which they used alcohol or other drugs, is a core identity feature. The vast majority of people who are in recovery define it in terms of abstinence. [11] While the road to recovery is varied, its destination clearly is long and sustained abstinence.
The recent emergence of the national recovery movement is one of the most positive changes in the nation’s long-term battle to overcome addiction. IBH encourages an open dialogue with people in recovery from substance use disorders to ask how they define “recovery” and how they achieved it. Stories of recovery often come in three parts: first, what life was like when a person was using; second, what happened to get the person to make the transformation into recovery; and third, what life is like in recovery. These are inspiring stories. The testimony of people in recovery is clear and convincing.
Conclusion
With the publication of Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health, the Office of the Surgeon General has catalyzed and challenged the nation to constructively confront the drug epidemic. We encourage national leaders and organizations that focus on substance abuse prevention and treatment to read the Report carefully and to consider our formulations of the fundamental goals of prevention and treatment and our related recommendations. Then we ask them to assess and redouble their commitment to prevention, treatment and recovery. Together we will heed and strengthen the Surgeon General’s most important messages: substance use is preventable and treatment leading to sustained recovery is possible.
Robert L. DuPont, MD, President, Institute for Behavior and Health, Inc.